Most people picture narcolepsy as someone who falls asleep without warning mid-conversation, or slumps over their dinner plate. It makes for a memorable movie scene. It's also a shallow and misleading picture of a complex neurological disorder that affects roughly 1 in 2,000 Americans and, on average, goes undiagnosed for 10 to 15 years after symptoms first appear.
The delay isn't because the symptoms are subtle. It's because they're misread: as depression, laziness, epilepsy, psychiatric illness, or simple tiredness. People lose jobs, relationships, and years of quality of life waiting for a diagnosis that, once found, finally explains everything.
If you or someone you love experiences overwhelming daytime sleepiness that doesn't respond to adequate nighttime sleep, this guide is worth reading carefully.
What Narcolepsy Actually Is
Narcolepsy is a chronic neurological disorder caused by the brain's inability to regulate the sleep-wake cycle properly. The underlying mechanism in the most common form, Type 1 narcolepsy, is the loss of neurons that produce hypocretin (also called orexin), a neuropeptide that acts as a stabilizer for wakefulness. Without enough hypocretin, the boundary between sleep and wakefulness becomes unstable. Sleep intrudes into waking life. Elements of REM sleep bleed into consciousness. The normal architecture of nighttime sleep is fragmented.
Narcolepsy is not a character flaw, a lack of effort, or the result of not sleeping enough at night. It is a permanent neurological condition with no cure, but one that can be very effectively managed with the right treatment and specialist care.
The Two Types
Type 1 Narcolepsy (with cataplexy): The classic form, defined by excessive daytime sleepiness plus cataplexy (described below). Caused by the loss of hypocretin-producing neurons, almost certainly through an autoimmune process. Hypocretin levels in cerebrospinal fluid are very low or undetectable.
Type 2 Narcolepsy (without cataplexy): Excessive daytime sleepiness without cataplexy, and with normal or near-normal hypocretin levels. The mechanism is less well understood. Some patients with Type 2 may later develop cataplexy and be reclassified as Type 1.
The Core Symptoms
Narcolepsy is a syndrome, not a single symptom. The full picture is distinctive, but symptoms rarely all appear at once or at the same severity, which is one reason diagnosis takes so long.
Excessive Daytime Sleepiness (EDS)
This is the cardinal symptom, present in virtually everyone with narcolepsy. But "sleepy" undersells it. People with narcolepsy describe a relentless, almost crushing need to sleep that descends without warning, regardless of how long or well they slept the night before.
Unlike the post-lunch dip most people feel, EDS in narcolepsy is pervasive and disabling. It strikes during active tasks, conversations, meals, and driving. Many people take multiple short sleep attacks in a day. Crucially, these episodes are often irresistible, not just "I feel tired."
After a brief sleep (even 5 to 20 minutes), people with narcolepsy typically feel refreshed, but only for a short time before sleepiness returns. This temporary relief from napping is actually a diagnostic clue that distinguishes narcolepsy from other causes of hypersomnia.
Cataplexy
Cataplexy is pathognomonic for Type 1 narcolepsy, meaning its presence is essentially diagnostic on its own. It is sudden, temporary muscle weakness triggered by strong emotion, most often laughter, excitement, surprise, or anger.
Episodes vary widely in severity:
- Mild: A fleeting weakness in the face (drooping eyelids, jaw slack, slurred speech), a buckling of the knees, or a dropping of the head
- Moderate: Weakness in the arms and legs, difficulty speaking or moving
- Severe: Complete muscle paralysis lasting up to a couple of minutes, with the person conscious and aware throughout
What makes cataplexy especially hard to recognize is that mild episodes look nothing like popular depictions of narcolepsy. A person whose face goes slack for two seconds when they laugh at a joke may not connect that to a sleep disorder. The link between strong emotion and brief physical weakness is unusual enough that many patients have described it to doctors for years without anyone recognizing it.
During cataplexy, the person remains fully conscious. They can hear and understand everything happening around them, they just cannot move. This distinguishes it from seizures, fainting, or drop attacks.
Sleep Paralysis
Sleep paralysis is the experience of waking up (or, less commonly, falling asleep) unable to move or speak. It typically lasts from a few seconds to a couple of minutes. It can be accompanied by vivid, often frightening hallucinations.
Sleep paralysis occurs in a small percentage of the general population as an isolated phenomenon. In people with narcolepsy, it is much more common and tends to be more frequent.
Hypnagogic and Hypnopompic Hallucinations
These are vivid, often realistic hallucinations that occur at the edges of sleep: when falling asleep (hypnagogic) or waking up (hypnopompic). They can be visual, auditory, or tactile, and are often described as deeply realistic and sometimes terrifying. A figure in the room. Sounds of someone entering the house. A physical sensation of being touched or held down.
These experiences, especially in combination with sleep paralysis, are frequently misinterpreted as psychotic episodes, ghost sightings, or alien abduction, and have historically led to misdiagnosis of schizophrenia or other psychiatric conditions.
Disrupted Nighttime Sleep
Despite their overwhelming daytime sleepiness, people with narcolepsy often sleep poorly at night. Their sleep is fragmented, with frequent awakenings. They enter REM sleep unusually quickly (often within minutes rather than the normal 90-minute delay), and their sleep stages are disorganized.
This is an important, often overlooked point: narcolepsy is not "sleeping too much." It's sleeping at the wrong times and in a disorganized pattern, with daytime sleep intrusion as a consequence.
Automatic Behaviors
During episodes of severe sleepiness, some people with narcolepsy continue performing routine tasks without awareness, what clinicians call automatic behavior. A person might keep writing, driving, or talking, but what they produce is garbled or makes no sense. They have no memory of the episode afterward. This is the result of partial sleep intrusion during an activity, and it can be dangerous, particularly when driving.
How Narcolepsy Is Diagnosed
There is no blood test for narcolepsy (except in some research settings). Diagnosis relies on clinical evaluation, sleep testing, and, in some cases, analysis of cerebrospinal fluid. The process has specific steps.
Step 1: Clinical Assessment
A sleep specialist takes a detailed history of your symptoms, including when they started, how often they occur, and what triggers cataplexy if present. You'll likely complete standardized questionnaires:
- Epworth Sleepiness Scale (ESS): Rates how likely you are to doze in 8 common situations. Scores above 10 suggest clinically significant sleepiness.
- Stanford Sleepiness Scale
- A detailed sleep diary, often for 1 to 2 weeks before testing
The specialist will also rule out other causes of daytime sleepiness: untreated sleep apnea, insufficient sleep syndrome, depression, thyroid disorders, or medication effects.
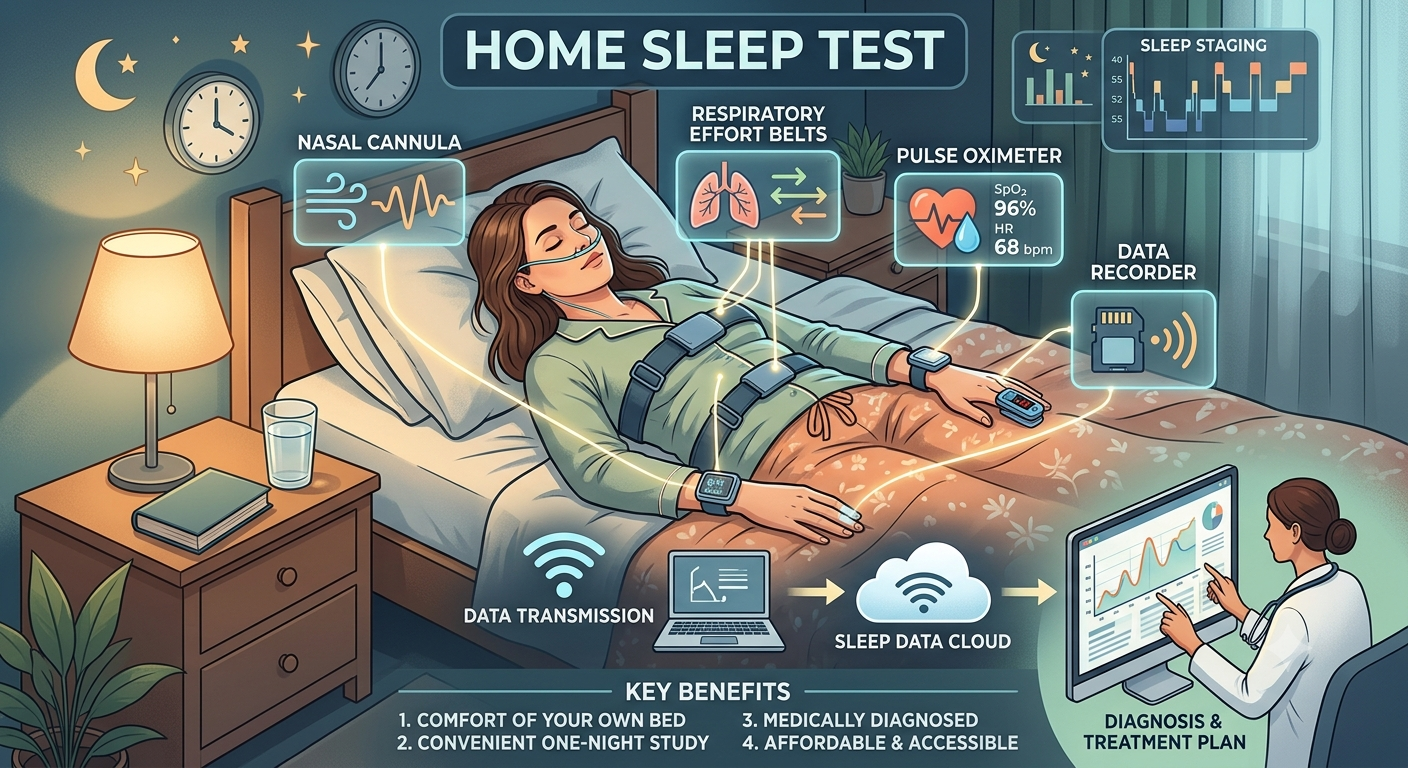
Step 2: Overnight Polysomnography (PSG)
Before the definitive narcolepsy test, you'll have a full overnight sleep study. This does two things:
- Rules out other sleep disorders (particularly sleep apnea) that could be causing the sleepiness
- Provides a baseline for the test that follows
The PSG is done in a sleep lab, with electrodes monitoring brain waves, eye movements, muscle activity, breathing, oxygen levels, and leg movements. You need an adequate night of sleep (at least 6 hours) for the next step to be valid.
Step 3: Multiple Sleep Latency Test (MSLT)
The MSLT is the core diagnostic test for narcolepsy. It follows immediately after the overnight PSG. Over the course of the day, you're given 4 to 5 nap opportunities, each 20 minutes long and spaced 2 hours apart. Technologists monitor what happens.
The test measures two things:
Sleep latency: How quickly do you fall asleep? An average sleep onset under 8 minutes suggests pathological sleepiness. Under 5 minutes is severe.
Sleep-onset REM periods (SOREMPs): Do you enter REM sleep within 15 minutes of falling asleep? In healthy sleepers, REM takes about 90 minutes. In narcolepsy, the brain plunges into REM immediately. Two or more SOREMPs across the nap sessions, combined with short sleep latency, strongly supports a narcolepsy diagnosis.
For the MSLT to be accurate, conditions matter enormously:
- You must not be sleep-deprived going in (hence the preceding overnight PSG)
- You must stop certain medications (antidepressants, stimulants, REM-suppressing drugs) typically 2 weeks before testing
- The test must be administered and scored by experienced technologists in an accredited lab
These requirements are also why DIY or home-based testing cannot diagnose narcolepsy, and why a mismanaged MSLT (wrong medication washout, inadequate prior sleep) can produce a false negative.
Step 4: Cerebrospinal Fluid Hypocretin Testing (Type 1 Only)
In select cases, a lumbar puncture can measure hypocretin-1 levels in the cerebrospinal fluid. Very low levels (below 110 pg/mL, or less than one-third of the normal mean) confirms Type 1 narcolepsy. This is especially useful when cataplexy is absent or unclear, or when the MSLT was inconclusive. It is not routinely done in straightforward cases.
Conditions Commonly Confused With Narcolepsy
Because diagnosis takes so long, it helps to understand what narcolepsy is mistaken for:
- Depression: Both cause fatigue and low motivation. But narcolepsy's sleepiness is neurological, not mood-related. Antidepressants prescribed for depression won't address the underlying problem and can interfere with accurate MSLT testing.
- Epilepsy: Cataplexy is sometimes mistaken for atonic seizures (drop attacks). But cataplexy is triggered by emotion and preserves full consciousness; seizures typically do not.
- Psychiatric illness: Hallucinations at sleep onset are sometimes read as psychosis. The sleep-edge context (and the person's otherwise intact cognition) is the distinguishing feature.
- Attention deficit disorder: Difficulty concentrating and staying engaged due to sleepiness resembles ADHD. Stimulant medications may even seem to help both conditions, further muddying the picture.
- Idiopathic hypersomnia: Another disorder of excessive sleepiness that lacks cataplexy and typically does not show SOREMPs on MSLT. Distinguishing it from Type 2 narcolepsy can be genuinely difficult.
Finding the Right Specialist
Not every doctor, and not every sleep specialist, is equally experienced with narcolepsy. Because it's relatively rare and the diagnostic pathway has specific technical requirements, the quality of care varies widely.
What to Look For
Board-certified sleep medicine physician. Look for certification from the American Board of Sleep Medicine (ABSM) or sleep medicine subspecialty certification through the American Board of Internal Medicine, American Board of Neurology, or another recognized board. This ensures training in the full spectrum of sleep disorders.
Neurologist or sleep physician with specific narcolepsy experience. Because narcolepsy is a neurological disorder, some of the most expert clinicians are neurologists who specialize in sleep, or sleep medicine physicians with a neurology background. Ask directly: how many narcolepsy patients does the practice see? This is a reasonable question that any experienced center should answer readily.
An accredited sleep center. The MSLT must be administered correctly to be valid. Labs accredited by the American Academy of Sleep Medicine (AASM) follow standardized protocols that affect the reliability of your results. Avoid unaccredited facilities for narcolepsy workups.
Ongoing management, not just diagnosis. Narcolepsy is a lifelong condition. The right specialist follows you over time, adjusts medications as needed, and stays current on new treatment options. A center that diagnoses and discharges is not enough.
Questions to Ask a Potential Provider
- How many patients with narcolepsy do you currently treat?
- Do you perform in-house MSLTs, and is your lab AASM-accredited?
- What is your medication washout protocol before the MSLT?
- Do you prescribe newer narcolepsy medications like sodium oxybate, solriamfetol, or pitolisant?
- How do you handle the distinction between Type 1 and Type 2 if cataplexy is atypical or borderline?
- Do you coordinate with neurologists when needed?
Patient Advocacy Resources
Narcolepsy Network (narcolepsynetwork.org) and Wake Up Narcolepsy (wakeupnarcolepsy.org) maintain provider directories and can help connect you with experienced clinicians. These organizations also have patient communities that are invaluable for sharing provider recommendations in your region.
What Treatment Looks Like
Narcolepsy has no cure, but with the right treatment most people can manage symptoms well enough to live full, active lives. Treatment is usually a combination of medication and behavioral strategies.
Medications for sleepiness:
- Modafinil and armodafinil (first-line, promote wakefulness with lower abuse potential)
- Solriamfetol (a newer option with strong efficacy data)
- Pitolisant (works via histamine, option for those who can't use stimulants)
- Amphetamine-class stimulants (methylphenidate, amphetamine salts) in refractory cases
Medications for cataplexy, sleep paralysis, and hallucinations:
- Sodium oxybate (Xyrem, Lumryz): the most effective treatment for cataplexy and also improves nighttime sleep and daytime sleepiness. Highly regulated due to its controlled-substance status.
- Pitolisant (also reduces cataplexy)
- Venlafaxine and other antidepressants (REM-suppressing properties reduce cataplexy, used as an alternative)
Behavioral strategies:
- Scheduled naps (2 to 3 brief naps daily can significantly reduce sleep attacks)
- Consistent sleep and wake times
- Avoiding alcohol and heavy meals during the day
- Workplace and school accommodations (narcolepsy is covered under the ADA)
- Strict caution about driving until symptoms are well controlled
The Bottom Line
Narcolepsy is one of the most misunderstood and underdiagnosed sleep disorders. Its symptoms are real, disabling, and have a neurological cause. They are not laziness, depression, or exaggeration. And for most people, the right diagnosis, when it finally comes, is not a life sentence but a turning point: the moment when the fog of a decade of confusion finally has an explanation, and treatment can begin.
If excessive daytime sleepiness is disrupting your life despite adequate sleep, or if you experience cataplexy, sleep paralysis, or vivid sleep-edge hallucinations, the path forward is a comprehensive evaluation at an accredited sleep center with a specialist experienced in disorders of hypersomnolence.
Don't wait another decade.
Ready to find a specialist? Use our sleep clinic directory to locate an accredited sleep center near you with board-certified sleep medicine physicians.
Written by
Daniel Marin
Sharing insights on sleep health and wellness to help you achieve better rest and improved quality of life.