It starts when you sit down to relax in the evening. A crawling, pulling, or itching sensation deep in your legs that you can't scratch or rub away. The only thing that helps is moving, so you get up. You walk around. It eases. You sit back down. It returns.
By bedtime, falling asleep feels almost impossible. You lie still, but your legs won't let you. You move them, and for a moment there's relief. Then the urge comes back. By 2 AM you're exhausted but still awake, still moving, wondering if this is just something you have to live with.
It isn't. What you're describing is almost certainly Restless Legs Syndrome (RLS), a genuine neurological disorder that affects an estimated 7 to 10 percent of adults in the United States. It is also one of the most underdiagnosed conditions in sleep medicine, partly because people assume restless, uncomfortable legs at night are just a quirk, and partly because the name makes it sound trivial.
It is not trivial. Untreated RLS can mean years of sleep deprivation, worsening mood, impaired concentration, and a significantly diminished quality of life. And for most people, it is very treatable once properly identified.
What RLS Actually Feels Like
The sensation of RLS is notoriously difficult to describe, which is one reason people hesitate to bring it up with a doctor. Common descriptions include:
- Crawling or creeping under the skin
- Pulling or tugging
- Itching deep inside the leg that can't be reached
- Electric or tingling sensations
- A "need to move" that is almost compulsive, not quite painful but deeply uncomfortable
The experience is often more of an urge than a pain. People say it feels like something is happening inside the leg, in the muscles or bones, not on the surface. It is not a cramp (which is involuntary and acute), not a numbness, and not typical tiredness.
Where It Occurs
RLS most commonly affects the lower legs, the calves and shins in particular. But it can also occur in the thighs, feet, and less commonly in the arms. When the arms are involved, the condition is sometimes called restless limb syndrome.
When It Strikes
Timing is one of the most distinctive features of RLS. Symptoms follow a clear circadian pattern: they are worst in the evening and at night, and minimal or absent in the morning. This pattern holds even in people who work night shifts and sleep during the day; the circadian clock, not the time on the clock, drives the cycle.
Symptoms are also triggered and worsened by rest and inactivity: sitting, lying down, long car rides, flights, movies, or any extended period of stillness. Movement, particularly walking, brings temporary relief. This relief-with-movement is a defining feature.
The Four Diagnostic Criteria
RLS is a clinical diagnosis, meaning it is based on your description of symptoms, not on a blood test or scan. The International Restless Legs Syndrome Study Group defines RLS by four criteria, all of which must be present:
- An urge to move the legs, usually accompanied by uncomfortable sensations
- The urge begins or worsens during rest or inactivity
- The urge is partially or fully relieved by movement
- The urge is worse in the evening or at night than during the day
If all four apply to you, you almost certainly have RLS. A fifth criterion, that the symptoms are not better explained by another medical or behavioral condition, helps rule out mimics.
RLS vs. Periodic Limb Movement Disorder
These two conditions are related but distinct, and they're worth understanding separately.
RLS is a conscious, subjective experience. You feel the urge and the discomfort. You move because you need to.
Periodic Limb Movement Disorder (PLMD) is characterized by involuntary, repetitive leg movements during sleep, typically a rhythmic flexion of the ankle, knee, and sometimes hip, every 20 to 40 seconds. These movements are recorded during a sleep study; you're usually not aware of them. Your bed partner, however, may be very aware.
About 80 percent of people with RLS also have PLMD, but many people with PLMD do not have RLS. PLMD can fragment sleep significantly, causing daytime fatigue even when you don't recall waking. A sleep study is the only way to detect and measure it, which is one reason a sleep specialist evaluation is valuable for RLS patients.
What Makes RLS Worse
Understanding your triggers helps with both self-management and discussions with your doctor.
Medications that commonly worsen RLS:
- Antidepressants (particularly SSRIs and TCAs, with the exception of bupropion which may actually help)
- Antipsychotics and some antiemetics (metoclopramide, promethazine)
- Antihistamines, including over-the-counter sleep aids like diphenhydramine (Benadryl)
- Lithium
If you take any of these and have RLS symptoms, it is worth raising this with your prescribing physician before assuming you need RLS-specific medication.
Lifestyle and dietary factors:
- Caffeine, especially in the afternoon and evening
- Alcohol, which may temporarily ease symptoms but worsens them later in the night
- Sleep deprivation (a vicious cycle: RLS disrupts sleep, and poor sleep worsens RLS)
- Prolonged sitting or inactivity
Medical conditions that worsen or cause RLS:
- Iron deficiency (even without frank anemia, low ferritin is a common, treatable trigger)
- Chronic kidney disease, especially end-stage renal disease
- Pregnancy (RLS affects up to 25 percent of pregnant women and typically resolves after delivery)
- Peripheral neuropathy
- Parkinson's disease
Iron deficiency deserves particular emphasis: it is one of the most common, most overlooked, and most treatable contributors to RLS. Many patients improve significantly once their ferritin level is brought up, sometimes without any RLS-specific medication at all. Standard iron panels can miss this because serum iron and hemoglobin can be normal while ferritin is low. Ask specifically for a ferritin level if you haven't had one checked.
When Self-Management Is Enough
Mild, occasional RLS, symptoms that occur a few times a month and don't significantly disrupt sleep, can often be managed without a specialist visit. Strategies that help many people:
- Avoiding caffeine and alcohol, particularly in the hours before bed
- Maintaining a consistent sleep schedule
- Moderate daily exercise (but not vigorous exercise close to bedtime, which can trigger symptoms)
- Warm baths or heating pads applied to the legs in the evening
- Leg massage
- Mental engagement (puzzles, games) during periods of forced inactivity like flights
- Reviewing medications with your doctor for any that may be contributing
If these measures bring your symptoms down to a manageable level and your sleep is not significantly affected, watchful waiting with lifestyle adjustments is reasonable.
When It's Time to See a Sleep Specialist
Self-management has a ceiling. Here are the signs that it's time to get professional help.
Your sleep is consistently disrupted. If RLS symptoms regularly delay your sleep, wake you repeatedly, or leave you exhausted in the morning, that's not something to push through. Chronic sleep deprivation compounds over time and affects every area of your health.
Symptoms occur most nights. Occasional RLS is uncomfortable. Daily RLS is a medical condition that warrants evaluation and, usually, treatment.
Your bed partner is affected. Periodic limb movements, which often accompany RLS, can disturb a partner's sleep significantly. A sleep study can document the extent of these movements and guide treatment.
You're pregnant and symptoms are severe. RLS in pregnancy is common and often resolves postpartum, but when it is severe enough to prevent sleep during an already-demanding time, a specialist can advise on the limited but real options that are safe during pregnancy.
You have kidney disease, neuropathy, or Parkinson's. Secondary RLS in these conditions tends to be more severe and requires specialist management coordinated with your other care.
You've tried self-management for weeks without improvement. If lifestyle changes haven't moved the needle, pursuing evaluation is the right call.
You're relying on over-the-counter antihistamines to sleep. These medications (diphenhydramine) worsen RLS and build tolerance quickly. If you've reached for them regularly, it's a sign the underlying problem needs to be addressed, not masked.
You've been told you kick in your sleep. Witnessed limb movements during sleep, or a bed partner who's been kicked awake, are red flags for PLMD. A sleep study can quantify and diagnose this.
What to Expect at a Sleep Specialist Appointment
A sleep medicine physician or neurologist with sleep expertise will:
- Take a detailed symptom history, including onset, frequency, timing, and what relieves or worsens symptoms
- Review your current medications for potential contributors
- Order blood work, including a ferritin level, iron studies, kidney function panel, and sometimes a complete blood count
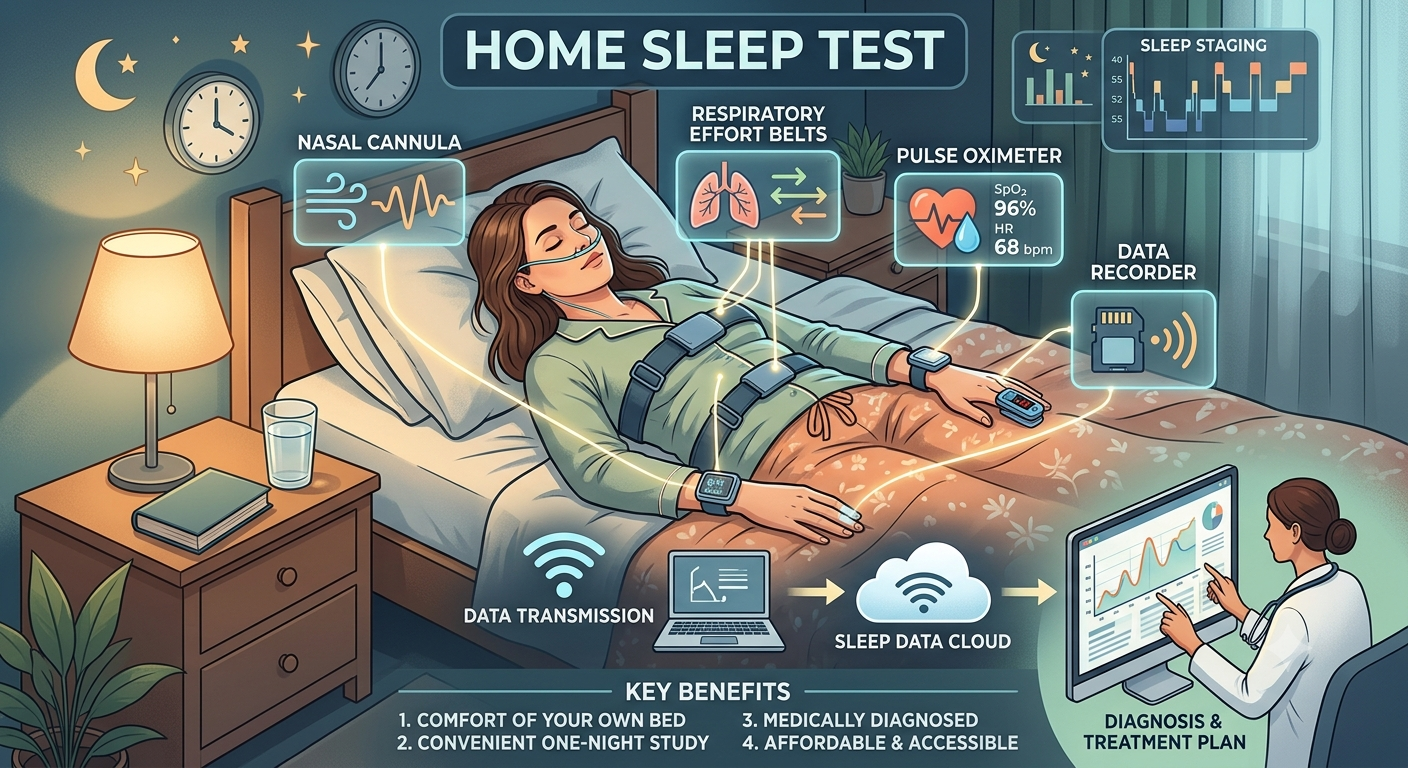
- Assess whether a sleep study is indicated to look for PLMD and to rule out other sleep disorders like sleep apnea (which commonly coexists with RLS)
Diagnosis is typically made at the first visit if your symptoms match the criteria. The conversation then moves quickly to treatment options.
How RLS Is Treated
Treatment depends on severity, underlying causes, and individual factors. A specialist will tailor a plan, but here's the general framework.
Correcting Iron Deficiency
If ferritin is below roughly 75 mcg/L (some guidelines use a higher threshold for RLS), iron supplementation is the first step. Oral iron is tried initially; intravenous iron is used when absorption is poor or symptoms are severe and need faster correction. This alone can substantially improve or resolve symptoms in iron-deficient patients.
First-Line Medications
For moderate to severe RLS, the two preferred medication classes are:
Alpha-2-delta ligands (gabapentin, pregabalin, gabapentin enacarbil): Now considered first-line by most guidelines. They reduce the sensory discomfort and urge to move, improve sleep quality, and carry no risk of augmentation (see below). Side effects include drowsiness and dizziness.
Dopamine agonists (pramipexole, ropinirole, rotigotine patch): Highly effective and fast-acting, but carry a risk of augmentation with long-term use. Once the most common first-line choice, they are now used more selectively due to augmentation concerns.
Augmentation: The Key Risk with Dopamine Agonists
Augmentation is a paradoxical worsening of RLS that occurs with long-term dopamine agonist use. Symptoms begin appearing earlier in the day, spread to more body areas, and become more intense even as the dose is increased. It affects a significant percentage of patients on these medications over several years.
This is not a reason to avoid dopamine agonists entirely, they work very well for many people, but it's a reason to start at the lowest effective dose, monitor carefully, and discuss augmentation risk with your prescriber. If augmentation develops, switching to an alpha-2-delta ligand or adding low-dose opioids (in severe refractory cases) may be needed.
Other Options
- Low-dose opioids (oxycodone, methadone, tramadol) for refractory or severe RLS unresponsive to other treatments
- Clonazepam for sleep maintenance, though not primarily for RLS symptoms
- Bupropion as an antidepressant option that does not worsen RLS
Finding the Right Provider
RLS sits at the intersection of sleep medicine and neurology. You may be evaluated by:
- A sleep medicine physician, who can diagnose RLS, order the necessary blood work and sleep study, and manage most cases
- A neurologist, especially if the picture is complex, secondary to a neurological condition, or refractory to first-line treatments
Look for a provider affiliated with an AASM-accredited sleep center. Ask whether they are comfortable managing RLS augmentation and refractory cases, and whether they have experience with IV iron infusion referrals for iron-deficient patients.
Your primary care doctor can initiate the evaluation, check ferritin, and refer you appropriately. But if your symptoms are moderate to severe, or if a first course of treatment isn't working well, a specialist brings the depth of experience that makes a real difference.
The Bottom Line
Restless Legs Syndrome is real, common, neurological, and treatable. The combination of evening-onset symptoms, worsening with rest, relief with movement, and disrupted sleep is distinctive enough that most experienced clinicians recognize it immediately.
If that description matches your nights, you don't have to keep moving through the dark hoping it gets better. A straightforward evaluation, a ferritin check, and a conversation with a specialist who knows this condition can change the trajectory quickly.
Ready to find care? Use our sleep clinic directory to locate an accredited sleep center near you with physicians experienced in restless legs syndrome and related movement disorders.
Written by
Daniel Marin
Sharing insights on sleep health and wellness to help you achieve better rest and improved quality of life.